Shouldn’t women decide if women have midwives?
Two weeks ago, I was bumped from a national radio show (I still love you, Diane Rehm!) as a consumer advocate for a final panel that was made up of the president of the national organization for obstetricians, another obstetrician, a nurse midwife, and a reporter. (The show was postponed when another news story took precedence.) The choice of topic, midwifery, was precipitated by the new U.K. guidelines urging that healthy, low-risk women consider midwife-led, out-of-hospital options for birth as a safer alternative to hospital birth (see New York Times article here).(1)
Right before the producer was about to hang up in my first conversation with her, she mentioned they had some doctors to talk to before they’d know if I would fit on the panel. I thought, “Oh, here we go,” and asked, “Can I just say one more thing?”
I then said something along the lines of: “I know you have to talk to the doctors, because they’re the ‘experts,’ right? But this is the changing conversation in maternity care. Women are smart enough to make these decisions. Women have the right to make these decisions. Women want midwives.”
This isn’t the first time. The press, and many others, have long deferred to doctors about whether midwifery is a legitimate option for women. Just this month, a piece by the New York Times editorial board praised midwifery, but still referred to medical centers as “allowing” and “letting” midwives to have more room to work.(2) (See “The Way We Talk About Midwifery Care Matters” for some great comments on this language.)
It seems like a no-brainer to me that when we are talking about midwifery care, the conversation should be with women and midwives. But one thing I’m sure that the general public and the media don’t understand, when they are constantly deferring(3) to doctors on this issue, is that doctors are the main reason women don’t have midwives.
What Exactly is Midwifery?
It may be hard for those of us born and raised in the U.S. to wrap our heads around the fact that midwife-led care is the global Gold Standard for mother/baby health.(4) For just a moment, though, suspend what you think you know, and consider that the U.S. has a uniquely dysfunctional system of maternity care, along with some famously poor outcomes for mothers and babies.(5) It’s helpful, then, to look outside our own system to see how things can be done better.
This summer, The Lancet, an internationally respected medical journal, published a series on midwifery that urged a “system-level shift” from a “fragmented” pathology-based (medical) model to a team-based, multidisciplinary model, with midwives as “pivotal” to this approach.(6)
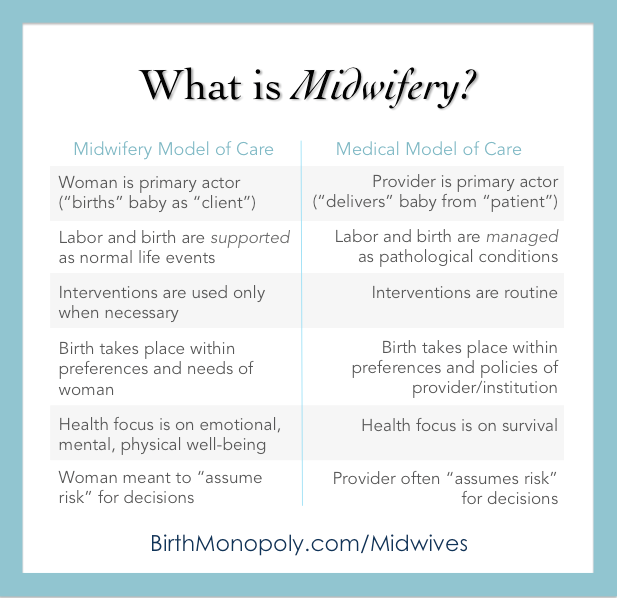
Midwifery is a model of care that predates and overlaps with medicine. It is, however, its own specialty: the specialty of supporting women in using their own bodies, brains, and strength to give birth. In midwifery care, birth depends less on interventions because it depends more on the capabilities of women. Midwives have “clients,” not “patients,” and a deep regard for women as the authorities on themselves and as the hearts of their families. Care is personalized, with face-to-face prenatal appointments often lasting 45 minutes or an hour each, and including information about nutrition and preparation for breastfeeding and the postpartum period. Of course, I am speaking generally here; there will be variations within the group. (Read this great article, “Comparing the Medical Model vs. Holistic Model…” for more.)
Midwives are trained to handle emergencies, focusing more on lower risk manual skills than technological ones, but some women and babies will need treatment–like surgery–that midwives don’t provide directly, but refer out to the appropriate specialist. This is where obstetrics comes in to complement and overlap.
Both professions are absolutely necessary, and the best scenario for families is one where midwives and obstetricians collaborate seamlessly, as a team. Women and babies benefit from top-notch prenatal care and the best chance of a healthy, uncomplicated birth, with the safety net of a specialized surgeon for the rare but real complications that may arise.
Bizarrely, however, the U.S. utilizes only these high-risk specialists (obstetricians) for almost everyone, even the huge number of women who would most benefit from the services of midwives. That number includes healthy women, but we have also seen that midwifery can help to mitigate risk in groups where the only difference between a small, sick, premature baby and a full-term, healthy one is an informed, supported mother. (Read about how one Florida Licensed Midwife is slashing preterm birth and Cesarean section rates in an at-risk community here; a Washington, D.C., birth center for low-income women does the same here.)
CLICK IMAGE TO SHARE ON FACEBOOK
Full-size, printable PDF at https://gum.co/midwives
To us in the U.S., the concept of autonomy for midwives or autonomy for women in childbirth is–largely–a foreign one. It is almost hard to imagine that a woman might independently choose to hire a midwife who works for herself or her own practice, and that the two of them together might decide when or if to bring in an obstetrician at any point. If that idea makes you uncomfortable, sit with it for a minute and think about why. What, or who, don’t you trust in that scenario?
A Conflict of Interest
In the early 1900s, the burgeoning American medical lobby was nearly successful in stomping out what they saw as their competition, including what the Journal of the American Medical Association and others called “the midwife problem,” through calculated smear campaigns. (Incidentally, in the same 1912 article I link to about “the midwife problem,” Dr. J. Whitridge Williams, an obstetrics professor at Johns Hopkins University, says that in a survey of obstetrics professors around the country, “a large proportion admit that the average practitioner, through his lack of preparation for the practice of obstetrics, may do his patients as much harm as the much-maligned midwife.”) Employing racist, sexist themes, this group portrayed midwives as unskilled, ignorant, and dirty. Up against the strategic efforts of moneyed white men to co-opt childbirth into an institutional model, midwives—disenfranchised, unrepresented, and powerless—didn’t have a chance. By the middle of the century, American birth had shifted from home to hospital, under the authority of doctors and leaving midwives (and poor, rural, and Black women) behind. (The crushing of the venerable Granny Midwife in the South deserves its own article.)

New England Journal of Medicine
The story of this shift is surprising and fascinating, and I encourage anyone who is interested to explore it: how an enterprising medical profession convinced women to give birth in institutions to be subjected to nonconsented medical experimentation and this: “at every level of predicted risk [for birth] measured, high and moderate as well as low, perinatal mortality was highest by far for births in hospitals and lowest for births at home.”(7)
Since then, midwifery has had to scrape and crawl its way back up to the present hodgepodge of different types of midwives, with various credentials and training, and a mishmash of state laws and rules that range from “Sure! Go get yourself a midwife!” to “If we catch you with a midwife, she’s going to jail.” Likewise, there’s a wide range of attitudes in the medical community about midwives, from beautiful medical-to-midwife collaboration, to punitive treatment of both midwives and their clients, as well as any physicians who dare to assist them. This article does not focus on the few places where collaboration is the rule of the day, but on the many places where it is not.
Things are better than they were, but nowhere near where they should be. Today, the American College of Obstetricians and Gynecologists (ACOG) refuses to recognize the midwives who attend around 80% of birth outside of hospitals(8) (“ACOG does not support programs that advocate for, or individuals who provide, home births.”)(9). They have only recently acknowledged “accredited birth centers” as acceptable locations, as their long-time policy has been that all birth should be hospital-based (a 2008 policy statement actually blustered, “Choosing to deliver a baby at home… is to put the process of birth over the goal of having a healthy baby”)(10). Thus, they do not embrace the position of their maternal health colleagues who believe all birth should be where women decide to give birth. There is truth to ACOG’s assertion that the training and education for a very small number of these midwives is not standardized, but, really, those midwives and their clients aren’t looking to obstetricians for approval. And pushing those midwives underground certainly does not result in better training or safer births.
One credential—that of Certified Nurse Midwife (CNM)—has found more acceptance in the medical community, but nurse-midwifery no longer resembles its origins of women on horseback delivering excellent care to the homes of other women in rural Kentucky. Now, 95% of nurse midwives work in hospitals,(11) most under—you guessed it—the supervision of doctors. Women aren’t just working with the midwife they’ve hired; they’re working with what the midwife’s backing physician, other physicians, and the institution will “allow.”
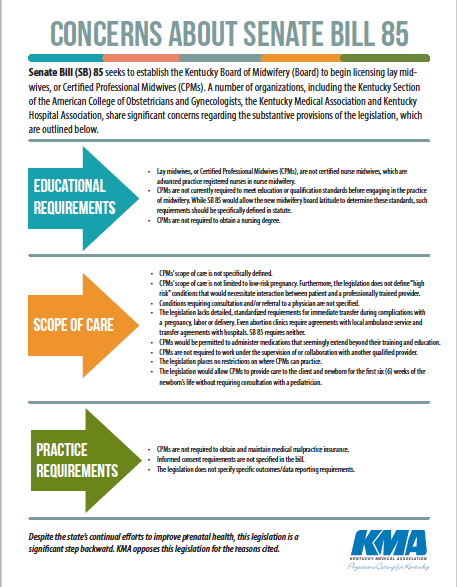
CLICK IMAGE TO SHARE ON FACEBOOK
Full-size, printable PDF at https://gum.co/midwives
It’s actually harder than you’d think to find places where a woman is free to independently hire and work with a midwife without the imposition of third-party supervision. Here’s one of many true stories about how this looks in real life, for one Certified Nurse Midwife: Midwife respects her clients’ right to give birth in whatever position they like, and knows that restricting women’s movement and positioning in labor and pushing can impede labor and injure women and babies. Random obstetrician from a different practice hears that midwife’s client gave birth on her hands and knees on a blanket on the floor. He complains to the hospital, triggering new policy. Now, Midwife’s clients must give birth in bed, like everyone else.
So, what does it matter that a woman has hired a midwife, when a random obstetrician she’s never even met can take her choice about how to give birth right out of her hands? This clues us in to why women are hiring midwives in the first place: we don’t always like to be told “how to give birth.”
No Way Out
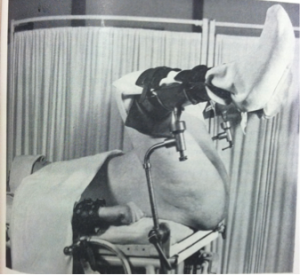
Lithotomy position from 1944 obstetric textbook. How much has changed, or not changed, in 70 years of better evidence and acknowledgement of human dignity?
Yes, most women are still being told how to give birth. They are subject to practices that have been proven harmful for decades: denying them food and drink in labor (60%), restricting them to bed (76%) on their backs (92%), and tying them to continuous electronic fetal monitoring (94%) that is so faulty, the U.S. Preventive Services Task Force issued a recommendation against it, as just a few examples (see State of Maternity Care Table)(12). In some facilities, policies of physical force are used when women don’t comply with provider preferences (see “Inappropriate Use of Restraints” for an all-too-typical example of the kinds of things I hear on a regular basis from consumers). Women are still having Cesareans in epidemic numbers, for things that evidence-based guidelines don’t support or that better care might have avoided (see ACOG Safe Prevention of the Primary Cesarean Delivery).
What happens to women who choose out-of-hospital care? It can be difficult for them to find doctors who will provide prenatal consultation, for one. Some women will forfeit their wish to give birth at home for fear of reprisals should they end up needing to transfer to a hospital in labor. I have spoken with women from all over the country who say they have been bullied, refused care, and treated with violence as home-to-hospital transfers. Louisiana mother Andrea Davis uses words like “violated,” “raped,” and “shame” to describe her experience (witnessed by her midwife, doula, husband, and seventeen-year-old daughter) after she transferred in to St. Tammany Hospital (which features a 45.1% Cesarean rate!) simply because she was exhausted after 24 hours of labor. Her story is not uncommon, and it’s not hard to understand why neither women nor their midwives would want to transfer into this kind of setting. It’s not hard to understand, either, why a woman wouldn’t choose that kind of environment for her birth in the first place.
Family doctors and obstetricians who support midwives and their clients may also face ostracism from their peers and their profession. Several who have contacted Improving Birth are worried they will lose their hospital privileges—and their practices—if they continue to collaborate with out-of-hospital midwives. It’s sad, because these collaborative relationships are exactly what make out-of-hospital birth safer.
Sociologist and professor of obstetrics and gynecology Raymond DeVries observes that other sociologists have “noted that licensing laws… have given professionals and their associations a restrictive monopoly over practice,” evolving from merely preventing an unlicensed person from using a certain title to making it “a criminal offense for the unlicensed to take any action specifically reserved for licensed professionals.”(13) He further notes the cozy relationship between the professional associations and the public agencies meant to act as regulatory and disciplinary bodies, quoting Ronald Akers’ study of the same: “It appears that their activities, personnel, and even finances overlap to such an extent that it is not entirely correct to say that the association ‘influences’ the board’s administration of public policy. . . . The cooperation between the two sometimes reaches the point of near identity.”(14) In other words, when medicine decided to “professionalize” childbirth, it simply staked out the boundaries and set up shop with the blessing of the state. The multibillion-dollar industry we have today has its roots in this self-defined, self-regulated system.
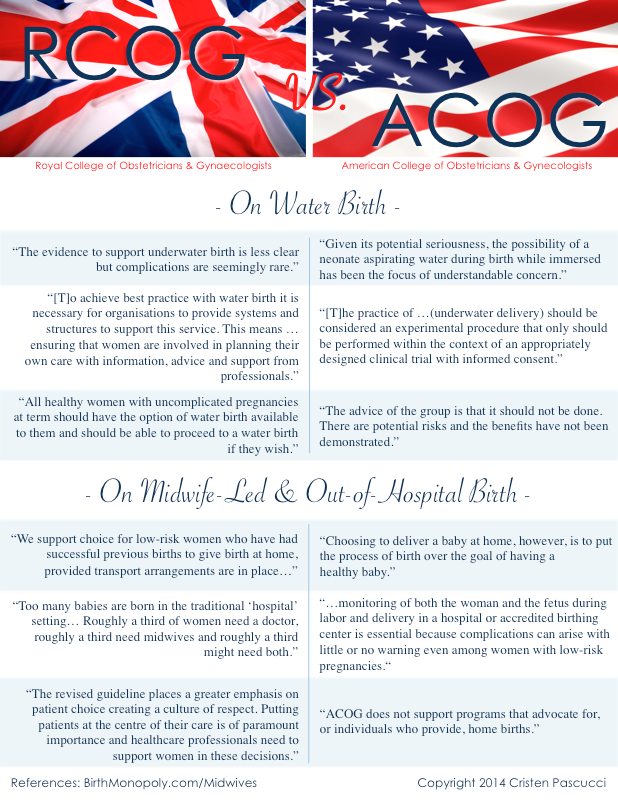
Indeed, when women have nowhere else to go, they are giving birth within the limits of what looks a lot like a monopoly: a profession answerable primarily to its own members, that sets its own standards for practice in an extraordinarily lucrative market, with no obligation to adhere to guidelines established by objective scientific organizations. Take a look at some of the differences between statements by the U.K. Royal College of Obstetricians and Gynaecologists on the one hand, and the U.S. ACOG on the other:
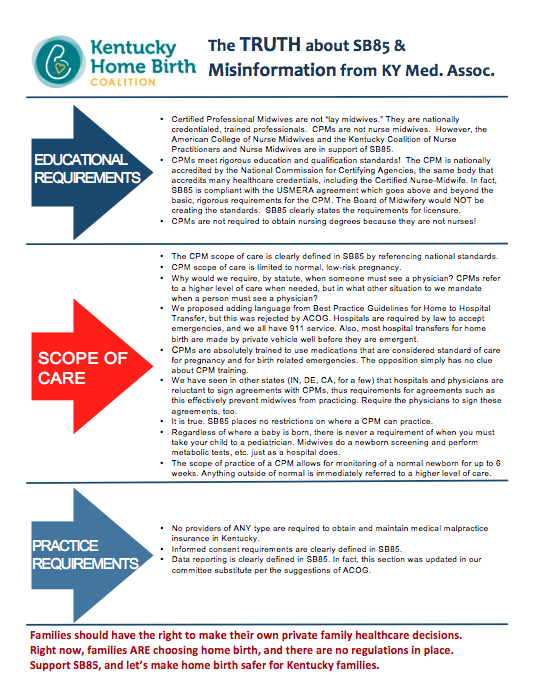
Click image for full-size, printable PDF from https://gum.co/midwives
Women vs. The Medical Lobby
The families are always caught in the middle: hurt by–and fed up with–a national maternity care system that Amnesty International calls a “crisis.”(15) Their frustration fuels grassroots efforts all over the country to reform, improve, and expand maternity care. But these consumer-fueled efforts routinely meet with opposition and resistance. You may be surprised to learn that this constant tug-of-war over the options available to women is between families and the medical lobby. Even as consumers beg for something different, the message they seem to keep getting is, “No–we know what’s best for you, and we’re it.”
Dozens of local and state consumer groups, as well as several national groups, are currently campaigning for more access to midwifery care. Certified Professional Midwives (CPMs) are legally allowed to practice in only 28 states; consumers in fourteen other states are actively working towards state licensure for CPMs, a formidable battle for what are often young, cash-strapped families. Their chief opposition? Doctors. The medical lobby. No other group is out there organized against access to midwifery, and it’s a powerful, well-funded group. In Alabama and Massachusetts, for example, the only opposition to proposed bills by consumer organizations (the Alabama Birth Coalition and Massachusetts Friends of Midwives) is the state medical society and state ACOG representation.
Ethicist and obstetrician/gynecologist Paul Burcher acknowledged this influence recently, as he urged his fellow doctors to reconsider their opposition: “Since obstetricians as a political lobby are largely responsible for these punitive laws [that make midwifery difficult to practice, or even illegal, in a home birth setting], we should work to have them overturned if we seek to renew the trust of our midwife colleagues” (emphasis added).(16)
Policing the Competition
Dr. Burcher is right. Even where midwifery is “legal” and licensed, it is frequently shaped by the political forces behind organized medicine. In other words, one profession is empowered by the state to police its competition. Its advice and permission are sought when the rules are made, and its presence—often a majority presence—is a given on the ruling bodies.
In Arizona, obstetricians are the reason a healthy woman MUST CONSENT to routine vaginal exams if she chooses an out-of-hospital midwife, because that’s one of the things the state ACOG representative pushed for in the rules. Now, if a woman does not consent in pregnancy and labor to routine vaginal exams—which are obsolete and even risky according to many practitioners, and painful and disruptive during labor—her midwife is legally obligated to drop the woman’s care and send her to an obstetrician for a hospital delivery. (The rules from the state of Arizona are here, but a more entertaining and pointed accounting from an actual midwife is here.)
I don’t know about you, but the idea that a vaginal exam is mandated by rule of the state is abhorrent to me. Put yourselves in those women’s shoes—er, stirrups. Can you imagine having to lie back and take a penetrating exam like that—just to retain the right to give birth outside of the hospital?
In Louisiana, the state with a 40% Cesarean rate,(17) if you’ve ever had a Cesarean birth, you actually have to get written approval from an obstetrician and apply on an individual basis to the state medical board (the medical board… of doctors) for permission to give birth at home with a midwife. You might argue that a woman who has had a Cesarean doesn’t fit a “low risk” profile qualifying her for an out-of-hospital birth, but here’s the dilemma for that same woman: also in Louisiana, if you’ve ever had a Cesarean, outdated policies and attitudes at most hospitals mean you’re not allowed to give birth vaginally there (in Ms. Davis’ parish, for example, the rate for vaginal birth after Cesarean is a depressing 1.5%).(18) The only way you are “allowed” to give birth is by surgery. By boxing women into hospital birth at facilities with mandatory surgery policies, the state medical board is essentially compelling Cesarean surgery for large groups of Louisiana women.
Consumer advocate and VBAC Facts founder Jennifer Kamel, who promotes access to accurate information about options for birth after a Cesarean, said: “I attended a California medical board meeting to speak as a consumer about restrictions on access to vaginal birth after Cesarean levied on women, whether they choose hospital or home. It is unbelievable to me that midwives have all of these regulations saying who they can/cannot see and when they need to refer out to a physician. However, when I asked the senior staff counsel for the medical board after the meeting if obstetricians had similar regulations that could say, mandate them to counsel women in a specific way about vaginal birth after Cesarean, or prohibit them/have repercussions for forced Cesareans, she informed me ‘no.’ [Over 40% of U.S. hospitals have mandatory surgery policies.] Fundamentally, this does come down to trust. The medical board does not trust midwives as a profession to make the right choice. And yet obstetricians have zero regulations comparable to midwifery regulations. They are trusted to determine when something is outside of their scope of practice and they need to refer her to another specialist. Midwives are not trusted.” (Ms. Kamel’s full statement to the board is here.)
These are the kinds of rules we get when a group is authorized by the state and the market to act in its own self interest to decide the “how, where, and with whom” about childbirth. What’s missing? The decisions of the women giving birth.
The Water Birth Debacle
Earlier this year, American medical organizations representing obstetricians (ACOG) and pediatricians (AAP) released a statement calling the safety of water birth into question, and advising that it should only take place as “an experimental procedure.”(19) It was an odd choice of subject, since water birth is almost exclusively a midwifery practice, especially when one statement author further explained that the statement was partially a response to what they believed was a proliferation of water births at home.(20)
The statement was full of scientific errors and misrepresentations, and excluded high-quality studies on tens of thousands of births. It warned women that there were no maternal benefits to water birth—which was incredible to many women who had actually had water births and experienced its benefits firsthand (Improving Birth asked women, and got over 130 responses on its Facebook page by the next day, here). The idea of no maternal benefits was also incredible to anyone who looked at the full body of research on water birth, which shows significant reduction in and even elimination of the use of episiotomy.(21)
Hospitals quickly shut down water birth programs even as consumers and midwives flooded ACOG and AAP with requests to take a scientific look at all of the evidence (read a letter from consumers here). From their noncommittal response, it does not appear that ACOG and AAP ever did so. The voices of women had no place in this discussion even as their births were the center of the debate. (In an interesting twist, the whole incident seemed to create a new crop of home birth families, because some women planning hospital water births moved those plans into their own homes.)
Evidence Based Birth’s Rebecca Dekker, PhD, RN, APRN, conducted a thorough review of the evidence (here). She commented: “I’m puzzled as to why keeping women’s perineums intact and uncut is not perceived as a benefit by anyone other than the women themselves. … Who should be weighing the potential harms and the potential benefits of waterbirth, and making an informed decision about their options? Should it be the mother? Or should it be the obstetrician?”(22)
On the other side of the ocean, the U.K.’s Royal College of Midwives (RCM) called the U.S. statement “disappointingly biased, and partially incorrect,” and asserted that women should not be denied an option for which no harms had been shown, especially considering that “Maternal choice in childbirth is a human right.”(23)

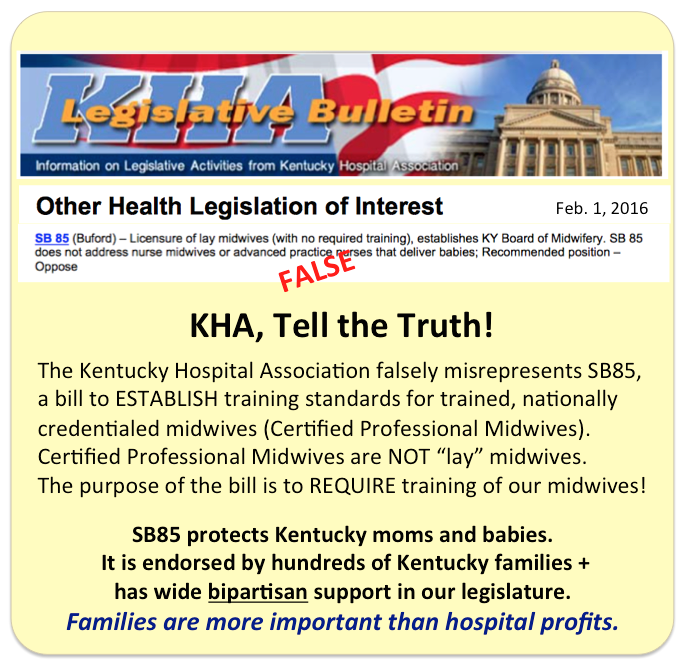
CLICK IMAGE TO SHARE ON FACEBOOK
Full-size, printable PDF at https://gum.co/midwives
Current U.K. guidelines from the RCM and the Royal College of Obstetricians and Gynaecologists state that because more research should be done on water birth, best practices are achieved by “ensuring that women are involved in planning their own care” and conclude that all healthy, low-risk women should have the option of water birth available to them.(24)
These disparate statements reflect the difference between a system that treats women as capable adults and one that sees them as being in need of instruction and authority. Now, I don’t doubt there are good intentions behind much of this paternalistic fuddy-duddying, but this kind of over-reaching is inappropriate in 2014 America. Worse, it’s harmful. Women like licensed midwife Jennie Joseph (British-trained, incidentally) have shown that compassionate, respectful midwifery care yields far superior health outcomes for underserved groups. Meanwhile, Black women and babies around the United States are dying at far higher rates than their white counterparts without that kind of care. (Here’s a story about Black women working to provide better care for their own communities, while having to fight the American Medical Association to do so.)
Before I end, I want to be clear about three things: One, I’m generalizing about entire professions, and I am deliberately highlighting the examples that prove my point (#notalldoctors!). ACOG has produced some wonderful work (like the “Safe Prevention” guidelines I mentioned earlier, or their amazing ethics guidelines). Obstetricians are a necessary and much-appreciated piece of the system, who are, moreover, under heavy pressures themselves. I work with some stellar ones who love and appreciate women and midwives. It is not every individual doctor, by any means, but the profession and its lobby that often acts as if the obstetrician in childbirth is there by right.
Two, there is no denying that American midwifery still needs developing, expanding, and organizing, including protections for consumers. But I am continually surprised by assertions that midwifery should be more hobbled in order to achieve these goals. I don’t see any efforts to restrict the profession of obstetrics, despite the critical state of maternity care today and reports from consumers all over the country about mandatory surgery policies, coerced procedures, and abuse in hospital-based settings–with no meaningful protections for consumers in place there, either. In fact, I believe that doctors would be very resistant to the idea of an outside party levying such restrictions. No; for midwifery to reach its potential, midwives must be recognized as autonomous professionals–self-defined and self-regulated.
Three, I’ve never had a home birth and never will. This has nothing to do with my personal choices. What I see is that midwifery care is the Gold Standard the world over, and the less than 10% of U.S. women taking advantage of it is an artificially low number. That number represents not women’s best interests, but a conflict between what women need and what Big Medicine already has.
Stay in Your Lane, Brother
The answer, when we keep asking doctors if women should have midwives (“Can we? May we? Should we?), is always going to be the same: “Maybe.” “Sometimes.” “As long as we’re supervising.”
In fact, one of the reasons it’s so refreshing to see the new guidelines from the U.K. is because they demonstrate a measure of trust in women and midwives that does not exist in the U.S. The new guidelines say, “You ladies can handle this. And if it gets hairy, you know we’re here for you.” The American attitude is quite the opposite: “You can’t handle this, and we’re going to impose our help whether you want it or not.”
This brings me back to my original question: Why are we asking doctors whether women can have midwives? Is it so hard to believe that women actually know what they need and want in childbirth? And that, for some of them, midwife-led care might be it?
Let’s please trust that women (#yesallwomen) are capable of figuring out how, where, and with whom to give birth. For those women who have the luxury of choice, they do not need to be told where to spend their maternity care dollars, nor do they deserve to have that money funneled into a system that doesn’t always fit them. For those women who are already limited in their choices, walling off an avenue for them to access compassionate, personalized, life-saving care is an egregious wrong. Finally, it is the human right of every woman to decide where, how, and with whom she will give birth. Period.
Moving forward, we must affirm that collaboration and respect among health care professionals can only make American maternity care better. A recognition of the natural rights of women over childbirth can only make care better. If it is midwives who women identify as best fitting their needs, that should be the end of the conversation. There is no other permission to be sought.
Cristen Pascucci (About the Author, Consult with the Author, Resources from the Author)
Founder, Birth Monopoly
Vice President, Improving Birth
Support my work + make change! Share this article with your legislators and state medical associations, as well colleagues and community members! Download the printer-friendly PDF of the article in its original form and in a “professional” version for distribution.
Also download these 8.5″x11″ handouts (below), for use with clients, colleagues, and friends.
Both resources are FREE (pay what you want) through January 15, 2015. Every dollar you give makes it possible for me to keep writing and providing free/low-cost resources to everyone.
Free or by credit card: CLICK HERE
By PayPal:
References: Article
(1) Bennhold, K., Saint Louis, C. (2014, December 3). British Regulator Urges Home Births Over Hospitals for Uncomplicated Pregnancies. The New York Times. (Article here.)
(2) Editorial Board. (2014, December 15). Are Midwives Safer Than Doctors? The New York Times. (Article here.)
(3) Valeii, K. (2014, December 17) How the Diane Rehm Show Perpetuates the Silencing of Women. Retrieved from BirthAnarchy.com. (Blog article here.)
(4) Sandall, J., Soltani, H., Gates, S., et al. (2013). Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database of Systematic Reviews, Issue 8. Art. No.: CD004667. DOI: 10.1002/14651858.CD004667.pub3. (Journal article here.)
(5) Amnesty International. (2010). Deadly Delivery: the Maternal Health Care Crisis in the USA. (Summary here. Download full report here.)
(6) Renfrew, M., McFadden, A., Bastos, M. (2014). Midwifery and quality care: findings from a new evidence-informed framework for maternal and newborn care. The Lancet, 384(9948), 1129 – 1145 (Abstract here. Download Executive Summary for series here.)
(7) Tew, M. (1998). Safer childbirth? A critical history of maternity care. (3rd Ed.). New York, NY: Free Association.
(8) MacDorman, M., Mathews, T.J., Declercq, E. (2014). Trends in out-of-hospital births in the United States, 1990–2012. NCHS data brief, no 144. Hyattsville, MD: National Center for Health Statistics. (Link here.)
(9) American College of Obstetricians and Gynecologists. (2008, February 6). ACOG Statement on Home Births. Retrieved from MedScape.com (Link here.)
(10) American College of Obstetricians and Gynecologists. (2008, February 6). ACOG Statement on Home Births. Retrieved from MedScape.com (Link here.)
(11) American College of Nurse-Midwives. (2014) CNM/CM-attended Birth Statistics. Retrieved from Midwife.org. (Link here.)
(12) Declercq, E., Sakala, C., Corry, M., et al. (2006, October). Listening to Mothers II: Report of the Second National U.S. Survey of Women’s Childbearing Experiences. New York: Childbirth Connection. (Link to report documents here.)
(13) DeVries, R. (1996). Making Midwives Legal: Childbirth, Medicine, and the Law. Ohio State University Press: Columbus.
(14) Akers, R. (1968). The Professional Association and the Legal Regulation of Practice. Law and Society Review 2: 463-82.
(15) Amnesty International. (2010). Deadly Delivery: the Maternal Health Care Crisis in the USA. (Summary here. Download full report here.)
(16) Burcher, P. (2014, December 4). What’s an Ethical Response to Home Birth? Retrieved from ObGyn.net. (Blog article here.)
(17) Arnold, J. (2013). Louisiana Hospital Cesarean Rates. Retrieved from CesareanRates.com. (Link here.)
(18) Louisiana Department of Health and Hospitals. St. Tammany Parish, Louisiana 2009-2011 Maternal and Child Health Profile. (Download report here. See all regional and parish-level data here.)
(19) American College of Obstetricians and Gynecologists Committee on Obstetric Practice and American Academy of Pediatrics. (2014, April). Committee Opinion No. 594, Immersion in Water During Labor and Delivery. Obstet Gynecol 2014;123:912–5. (Link here.)
(20) Stokowski, L., Macones, G. (2014, March 27). ACOG Rep Says Underwater Delivery Is a Bad Idea. Retrieved from MedScape.net. (Link here; website membership to view article is free.)
(21) Dekker, R. (2014, July 10). The Evidence on Water Birth. Retrieved from EvidenceBasedBirth.com. (Link here.)
(22) Muza, S. (2014, July 10). Evidence on Water Birth Safety–Exclusive Q&A with Rebecca Dekker on her New Research. Retrieved from ScienceandSensibility.org. (Blog article here.)
(23) Burns, E. (2014). Response to joint American College of Obstetricians and Gynecologists (ACOG), and American Academy of Pediatrics (AAP) Committee’s opinion regarding birthing pool use during labour and waterbirth. Retrieved from RCM.org.uk. (Download letter here.)
(24) Alfirevic, Z., Gould, D. (2006). Royal College of Obstetricians and Gynaecologists/Royal College of Midwives Joint statement No. 1, Immersion in Water During Labour and Birth. (Download guidelines here.)
References: “RCOG vs. ACOG” Handout
RCOG Statements:
“The evidence to support underwater birth is less clear…”
“[T]o achieve best practice with water birth…”
“All healthy women with uncomplicated pregnancies at term…”
Alfirevic, Z., Gould, D. (2006). Royal College of Obstetricians and Gynaecologists/Royal College of Midwives Joint statement No. 1, Immersion in Water During Labour and Birth. (Download guidelines here.)
“We support choice for low-risk women…”
Roberts, M. (2014, May 12). Labour wards not for straightforward births, says NICE. Retrieved from BBC.com. (Article here.)
“Too many babies are born in the traditional ‘hospital’ setting…”
Borland, S. (2011, July 15). Big push for home births: Too many babies are being born in hospital, say doctors. Retrieved from DailyMail.co.uk. (Article here.)
“The revised guideline places a greater emphasis on patient choice…”
Royal College of Obstetricians and Gynaecologists. (2014, December 3). RCOG statement on revised NICE intrapartum care guidelines. Retrieved from RCOG.org.uk. (Link here.)
ACOG Statements:
“Given its potential seriousness…”
“[T]he practice of …(underwater delivery)…”
American College of Obstetricians and Gynecologists Committee on Obstetric Practice* and American Academy of Pediatrics. (2014, April). Committee Opinion No. 594, Immersion in Water During Labor and Delivery. Obstet Gynecol 2014;123:912–5. (Link here.)
“The advice of the group is that it should not be done…”
Goldman, A. (2014, March 26). The New Warning About Water Births. Retrieved from WomensHealthMag.com. (Article here.)
“Choosing to deliver a baby at home…”
“… monitoring of both the woman and the fetus…”
“ACOG does not support programs that advocate for…”
American College of Obstetricians and Gynecologists. (2008, February 6). ACOG Statement on Home Births. Retrieved from MedScape.com (Link here.)
ACOG’s current policy on home birth is here (2011, reaffirmed 2013).
“You’re Not Allowed to Not Allow Me” is one of the essays in Take Back Your Birth, a 30-page eBook by Cristen Pascucci written to inspire and inform moms. It can be given as a gift to to-be mothers and is also appropriate for professionals to use with their clients.Click here to get yours!
“Take Back Your Birth is balanced, informative (evidence-based), simple and to-the-point, as well as encouraging and inspiring…all the while carrying a lighthearted and compassionate tone.” – Rachael Hutchins, Doula Rachael Birth Services, Woodstock, Georgia
[shareaholic app="share_buttons" id="6904933"]
}); } function mce_success_cb(resp){ $('#mce-success-response').hide(); $('#mce-error-response').hide(); if (resp.result=="success"){ $('#mce-'+resp.result+'-response').show(); $('#mce-'+resp.result+'-response').html(resp.msg); $('#mc-embedded-subscribe-form').each(function(){ this.reset(); }); } else { var index = -1; var msg; try { var parts = resp.msg.split(' - ',2); if (parts[1]==undefined){ msg = resp.msg; } else { i = parseInt(parts[0]); if (i.toString() == parts[0]){ index = parts[0]; msg = parts[1]; } else { index = -1; msg = resp.msg; } } } catch(e){ index = -1; msg = resp.msg; } try{ if (index== -1){ $('#mce-'+resp.result+'-response').show(); $('#mce-'+resp.result+'-response').html(msg); } else { err_id = 'mce_tmp_error_msg'; html = '
';
var input_id = '#mc_embed_signup';
var f = $(input_id);
if (ftypes[index]=='address'){
input_id = '#mce-'+fnames[index]+'-addr1';
f = $(input_id).parent().parent().get(0);
} else if (ftypes[index]=='date'){
input_id = '#mce-'+fnames[index]+'-month';
f = $(input_id).parent().parent().get(0);
} else {
input_id = '#mce-'+fnames[index];
f = $().parent(input_id).get(0);
}
if (f){
$(f).append(html);
$(input_id).focus();
} else {
$('#mce-'+resp.result+'-response').show();
$('#mce-'+resp.result+'-response').html(msg);
}
}
} catch(e){
$('#mce-'+resp.result+'-response').show();
$('#mce-'+resp.result+'-response').html(msg);
}
}
}
// ]]>